Expanding ERT indications and rising utilization make it increasingly difficult to justify nonhormonal trial participation. Symptomatic patients already on effective hormonal therapy are unwilling to discontinue, and investigators in ERT-saturated markets resist enrolling into protocols that compete with a well-established standard. The washout-tolerant eligible pool contracts silently.
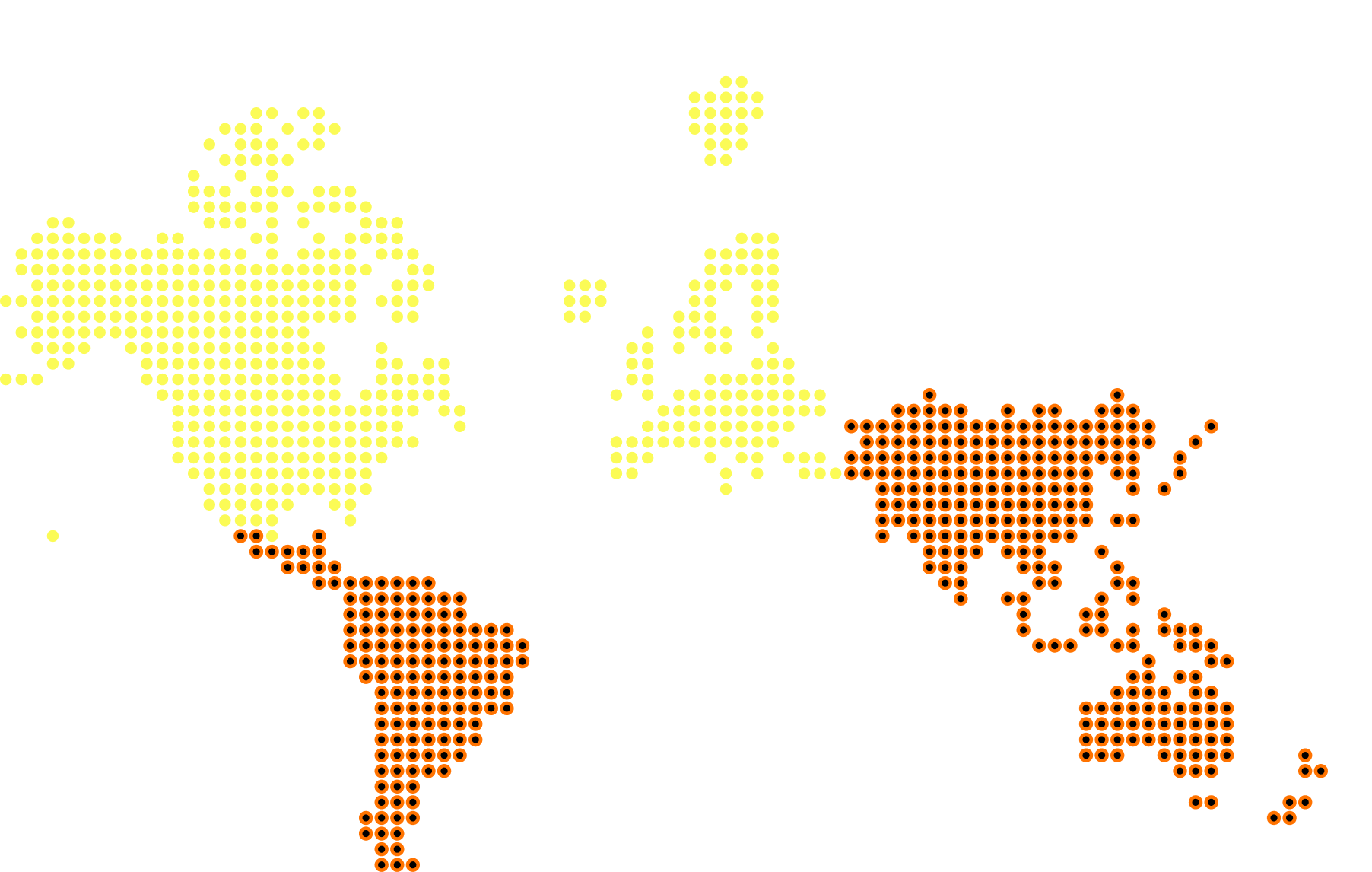
Lindus queries 40M+ EHR records to model the size and geographic distribution of ERT-contraindicated and ERT-averse subpopulations before protocol finalization, stress-testing washout viability against real-world prescribing trends. Patient concierge coordinators support identified candidates through washout: managing scheduling, transport, and symptom-rebound guidance to sustain enrollment in a shrinking eligible window.

.jpeg)